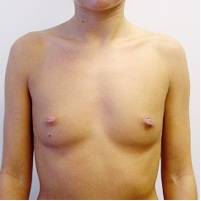
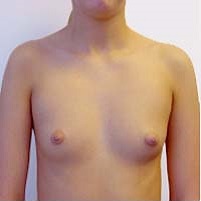
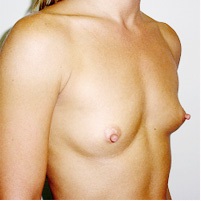
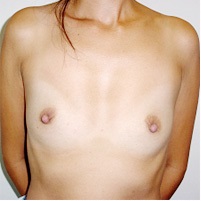
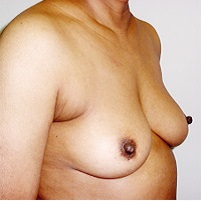
Before/After
20 yrs; endoscopic breast augmentation via armpit incision
46 yrs, 5'9", 140 lbs, 3 children; endoscopic breast augmentation via armpit incision with 350cc saline implants under the pectoralis muscle
20 yrs; endoscopic breast augmentation via armpit incision
38 yrs, 5'9", 140 lbs; endoscopic breast augmentation via armpit incision using 350cc saline implants under the muscle
34 yrs, 5'1", 97 lbs, 2 children; endoscopic breast augmentation via armpit incision using 300 cc saline implants under the pectoralis muscle
37 yrs, 5'4", 112 lbs, 1 child; endoscopic breast augmentation via armpit incision using 350cc saline implant left side & 330cc right side under the pectoralis muscle
38 yrs, 5'3", 98 lbs, 34AA cup before; endoscopic breast augmentation via armpit incision using 350cc saline implants under the pectoralis muscle
44 yrs, 5'6", 130 lbs, 2 children; endoscopic breast augmentation via armpit incision using 270cc saline implants under the pectoralis muscle
‹
›
What is an Augmentation Mammoplasty?
Augmentation Mammoplasty (Breast Augmentation) is a surgical procedure for the sole objective of enlarging the size of the breasts. Currently there is no diet, medications, hormones or exercises that will effectively increase breast size short of pregnancy or massive weight gain. The most practical method of enlarging the breasts is by insertion of a breast prosthesis consisting of a silicone envelope beneath the breast tissue. It is a very common operation, having been performed on well over a half million women in North America alone, over the last 20 years.
Who can benefit from this operation?
The three general groups of women that can benefit from this operation are those who have failed to ever develop adequate breast size, those who have lost breast fullness following pregnancy, weight loss, or age, and finally those women who have significantly different sizes of their breasts.
What can the operation achieve and what are the limitations?
The implant increases or restores lost breast volume. The operation does not affect the skin and therefore does not remove stretch marks. It increases volume and may disguise but does not correct breast droop or sag. It can often reduce but not totally eliminate pre-existing asymmetry. The size is increased but the general shape of the breast is unaltered. The margin of the implant is occasionally felt or seen as a wrinkle (especially with larger implants).
How does the body normally react to the prosthesis?
The body normally forms a thin layer of scar tissue around the silicone prosthesis enclosing it in a loose pocket that does not distort the implant shape and feels soft as a normal breast.
What happens with pregnancy?
The implant does not prevent lactation however not all women even without augmentation can breast feed. Following breast-feeding the breast tissue usually returns to pre-pregnancy size and normally sags.
What about the risk of breast cancer?
There is no relationship between implants and the development of breast cancer. The risk is neither increased nor decreased. The implant is behind the breast tissue and does not prevent detection of breast lumps, however investigation of the presence of a lump may be more complicated with an implant in place. Mammograms may be done, however, more X-ray views may be required and the implant may mask or distort the appearance of a cancer on a mammogram.
What are the choices of incisions, implant position and type of implant?
The three incisions available are around the areola (the dark area around the nipple), the fold beneath the breast, and in the armpit. The most common are the former two. The implant can be placed behind breast tissue or both pectoral muscle and breast. Each has advantages and this can be discussed with Dr. Horton. All implants are made of a silicone envelope and differ in the contents. Presently the only implants that can practically be inserted through the armpit are filled with saline (salt water). Similar to any mechanical device these may rupture due to injury or normal wear over time releasing the saline solution resulting in deflation and required removal.
How is the operation performed?
There are many variations of doing an augmentation mammoplasty as discussed above. Your preferences influence the decision-making. Dr. Horton prefers using an incision in the armpit or around the lower edge of the areola. The incision in the armpit provides access to the space between the breast and the pectoral muscle or beneath the muscle (see diagram). Through this incision the endoscope (surgical telescope) is introduced to develop the pocket for the implant. In most patients this leaves a permanent fine line scar in the armpit with no scars on the breast.

How is the size of the implant determined?
Dr. Horton will personally work with you to determine your best fit during your private consultation. The size of the implant will be personalized to fit with your goals and with your body. There are some physical limitations on the attainable size, basically related to the size of the breast's skin envelope. Previously stretched skin (as in post pregnancy breasts) will tolerate larger implants. In general, the larger the implants, the greater the risk of complications, as more surgery is required to develop a large pocket for an implant. It is important to realize too large an implant can be aesthetically unpleasing.
What can I expect as the usual post-operative recovery?
Postoperatively, a clear plastic bandage is applied to the skin. There is bruising and swelling for several weeks. Pain is usually moderate after the first day. Arm activity is markedly limited for the first week, with a gradual return to normal and vigorous activity after three to four weeks. You will be instructed to do breast massage daily to stretch out any developing fibrous tissue to minimize the chance of fibrous capsule contracture (see below).
What is the most common problem associated with the operation?
In 20 to 40% of patients the fibrous layer surrounding the implant can tighten and apply pressure to the outside of the implant. This "fibrous capsular contracture" causes the breast to feel unnaturally firm and appear too rounded. This is the most common complication of augmentation and can usually be dealt with by a simple manipulation in the office if done early. Certain patients may benefit from a secondary operative procedure to surgically release this fibrous layer. Some who are prone to this problem may continue to have firm breasts even after such secondary surgery. Rarely this is severe enough to make removal of the implants advisable.
What are the other common possible complications?
The complications of anesthesia, whether local or general, are part of the risk of even minor surgery. Breast augmentation is a relatively low risk procedure, but as with any operation, there are certain potential problems. The basic mechanisms of infection (which may require removal of the implant for treatment), bleeding, circulatory compromise to the skin, and poor or painful scar formation are complications in any surgery. Nipple sensation may be increased or decreased, which can be temporary or permanent. Stretch marks in the skin can occur. Calcium can form around the implant after many years. Asymmetrical positioning of the implants is uncommon and is usually due to some pre-existing breast asymmetry or shifting of the implant as the result of severe capsular contracture. Occasionally, usually due to infection, the implant may erode through the skin and be "rejected" by the body. Uncommonly the implants can rupture requiring removal and replacement of the implant. It is postulated that an autoimmune syndrome (Human Adjuvant Disease) may occur producing a Rheumatoid Arthritis, Systemic Lupus, or Scleroderma like condition. Any of these complications may result in temporary or permanent disability or deformity, may require further surgical treatment, and a possibly prolonged recovery period and time off work.